
The problem
Pre-authorization and referral submission lived in the membership view. A provider office picks a patient, then tries to submit an auth or referral to the plan. In one-on-ones, I watched office staff fight the form—too many options, unclear labels, everything mixed together.
I took that suspicion to our health plan partners. We reviewed their reports and sat with their workflow. The pain wasn’t theoretical.
“We spend about 50% of our time fixing authorizations rather than approving or denying them. I spend a lot of time on the phone with providers trying to help them submit correctly.” — Health plan partner
Research
I also brought in people who know pre-auth workflows but don’t live in our tool every day. They ran the current product and said the quiet part out loud:
“This list is ridiculous—which one is the right one? I’ll just pick this and write what I want in the comments.” — Usability session participant
Authorizations and referrals were jumbled. Staff couldn’t tell what the plan actually needed. Comments became a dumping ground for missing structure.
Hypothesis
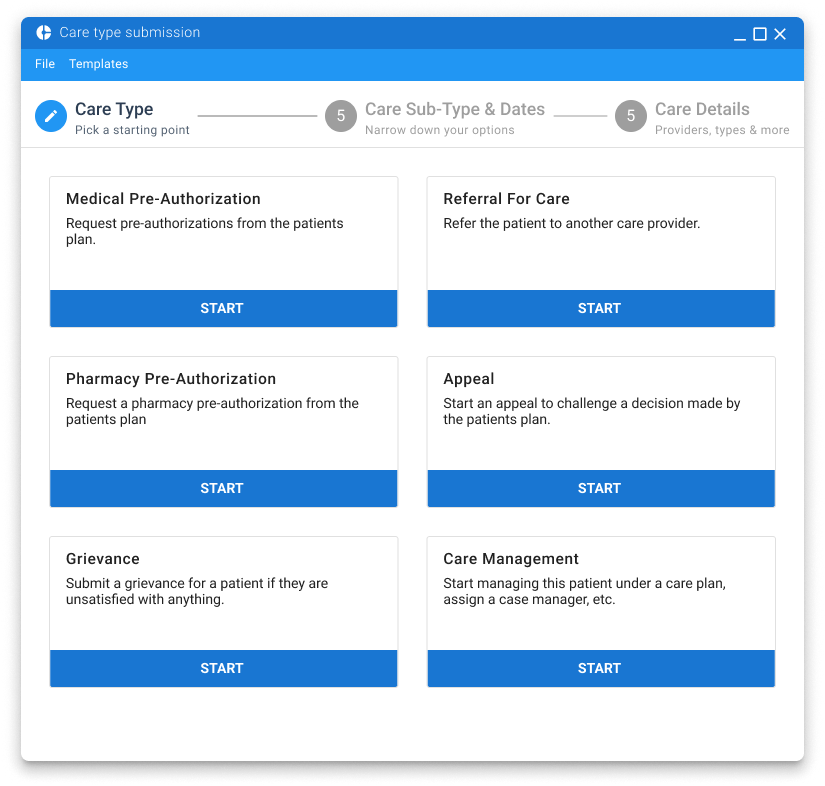
Segment pre-authorizations and referrals into clear care types (and sub-types) so the form only asks for data that type needs—and so the plan receives something they can act on.
Goal: fewer bad submissions, less plan-side rework and coaching.
What we built
Card sorting with plan partners and provider office staff: primary care types and sub-types. That segmentation powered a wizard-style stepper—each step controlled by the care type, not a single overloaded form.
We validated with prototypes (Sketch/InVision at the time), then refined through development with continuous usability checks.
Results
≈90% reduction in error-driven rework
From partner workflow reports after rollout; templates later cut provider time further.
Relative share of plan-side correction reasons before the redesign.
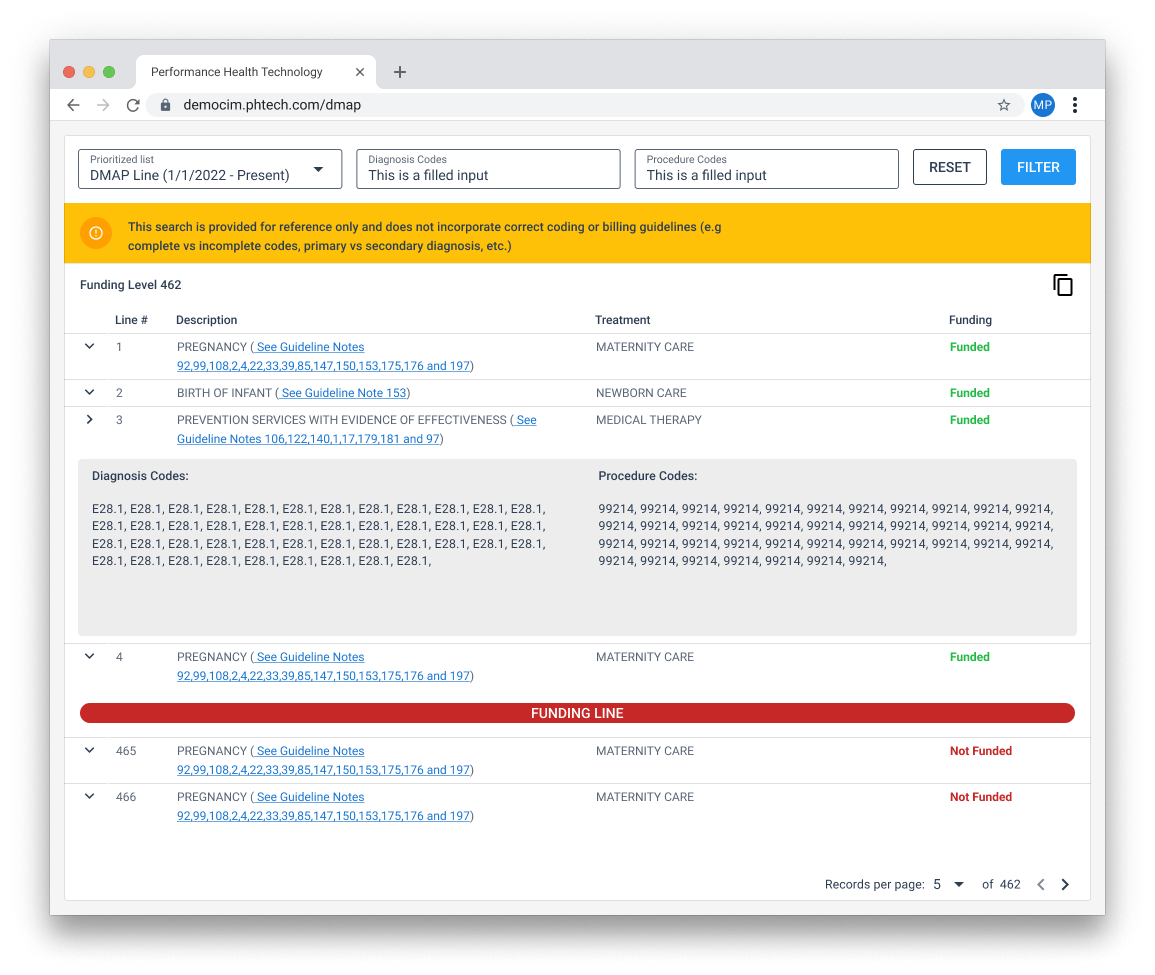
Feedback from plans and providers improved across the workflow. We later added templates to speed repeat submissions, and an ICD-10 lookup so offices can check billable codes without leaving the tool.
Why this still matters
Multi-step clinical and plan workflows fail the same way: too many choices, not enough structure, humans papering over the product in free text. Segmentation + guided steps is still how I approach dense healthcare forms—claims, auths, referrals, assessments.